Hamed Abbaszadegan, MD, MBA
May 30, 2026

The conversation about AI in medicine focuses on the wrong location.
Diagnostic algorithms in radiology departments. Drug discovery platforms in pharmaceutical labs. Surgical robots in operating rooms. These applications matter, but they reinforce the existing power structure. Healthcare institutions retain control. Patients remain dependent.
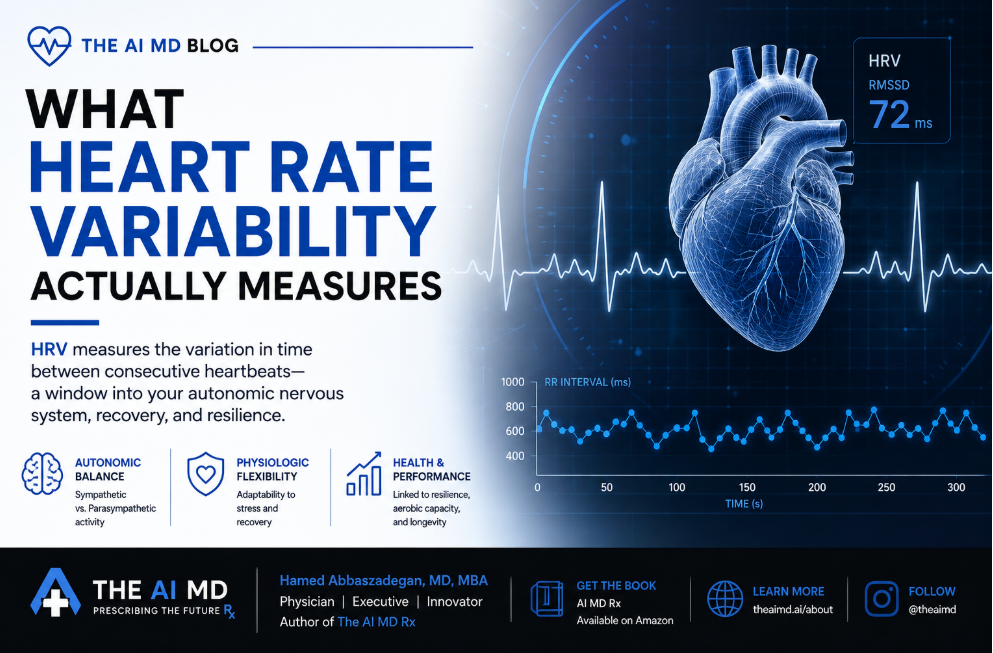
The actual transformation happens when someone checks their smartwatch at breakfast and understands what their heart rate variability means for their metabolic health three months from now.
That shift relocates medical agency from the doctor's office to the device on your wrist. It changes who owns health optimization. And it requires infrastructure that doesn't exist yet.
Wearable adoption increased from 30% in 2019 to 41% of U.S. households by March 2024. Global shipments reached 611.5 million units in 2025.
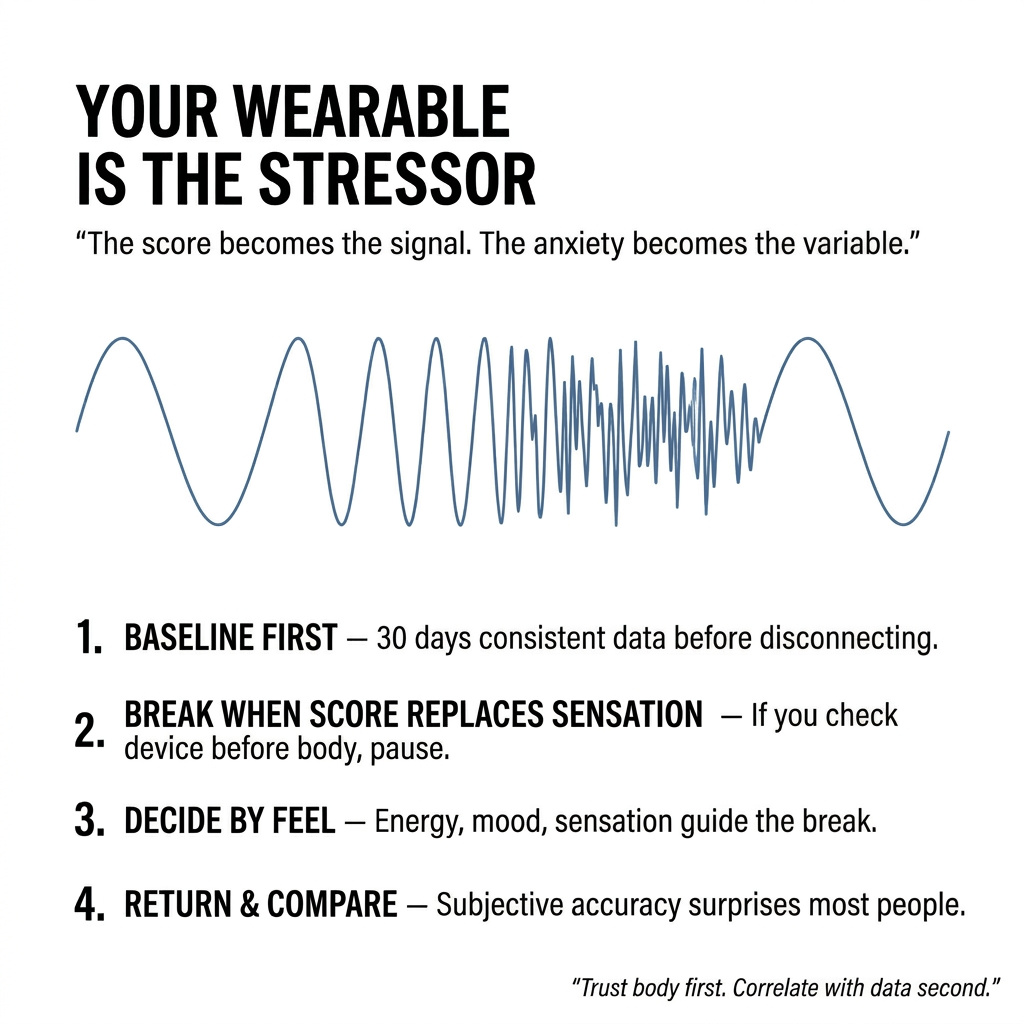
People own the devices. They generate the data. But ownership without interpretation creates noise, not insight.
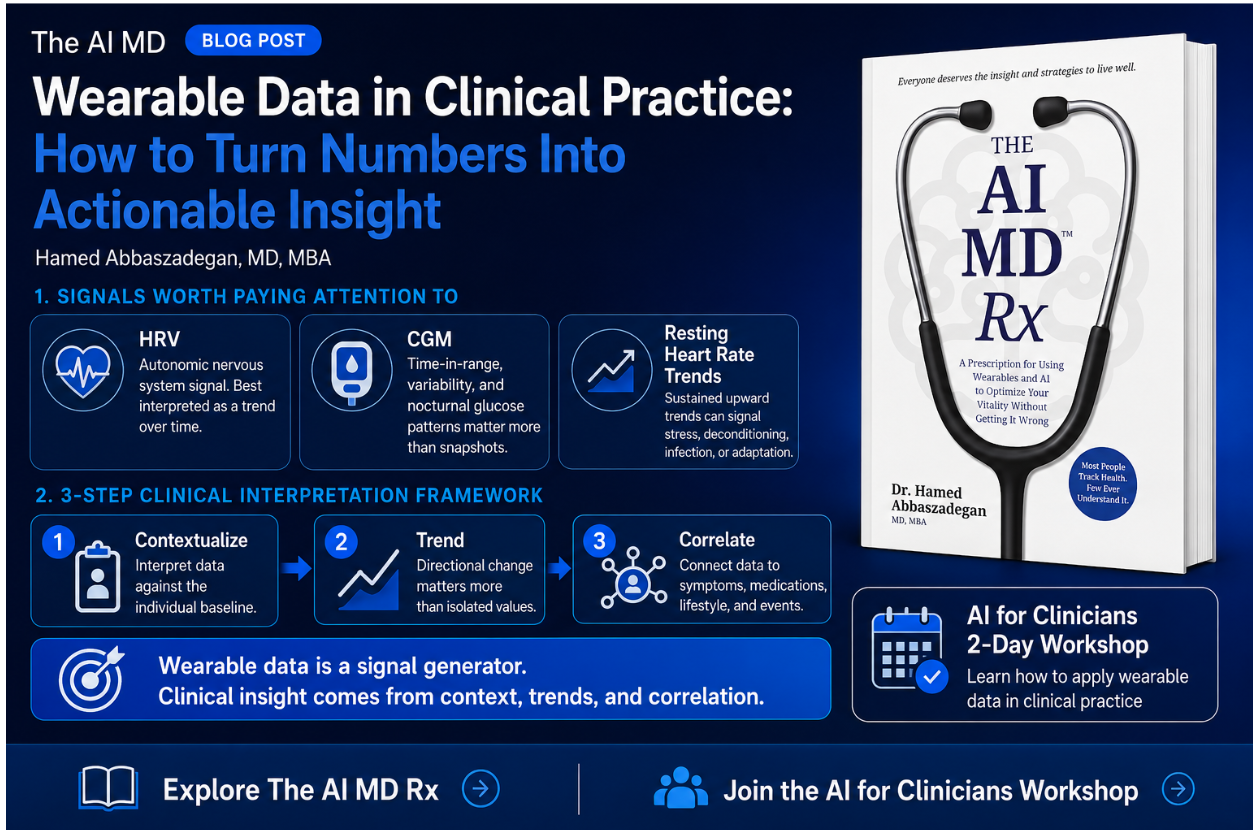
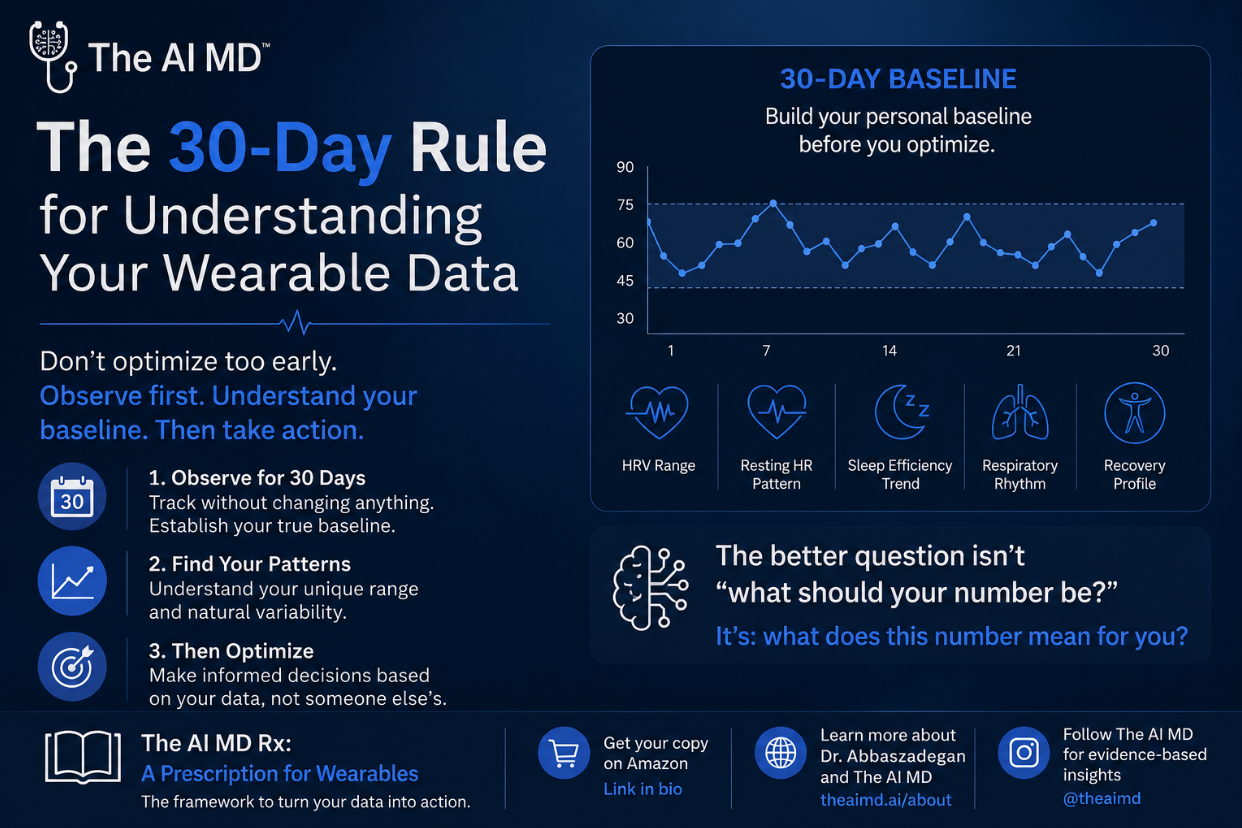
A typical smartwatch records tens of thousands of data points daily. Heart rate every second. Sleep stages throughout the night. Activity patterns across weeks. The volume overwhelms. The meaning remains hidden.
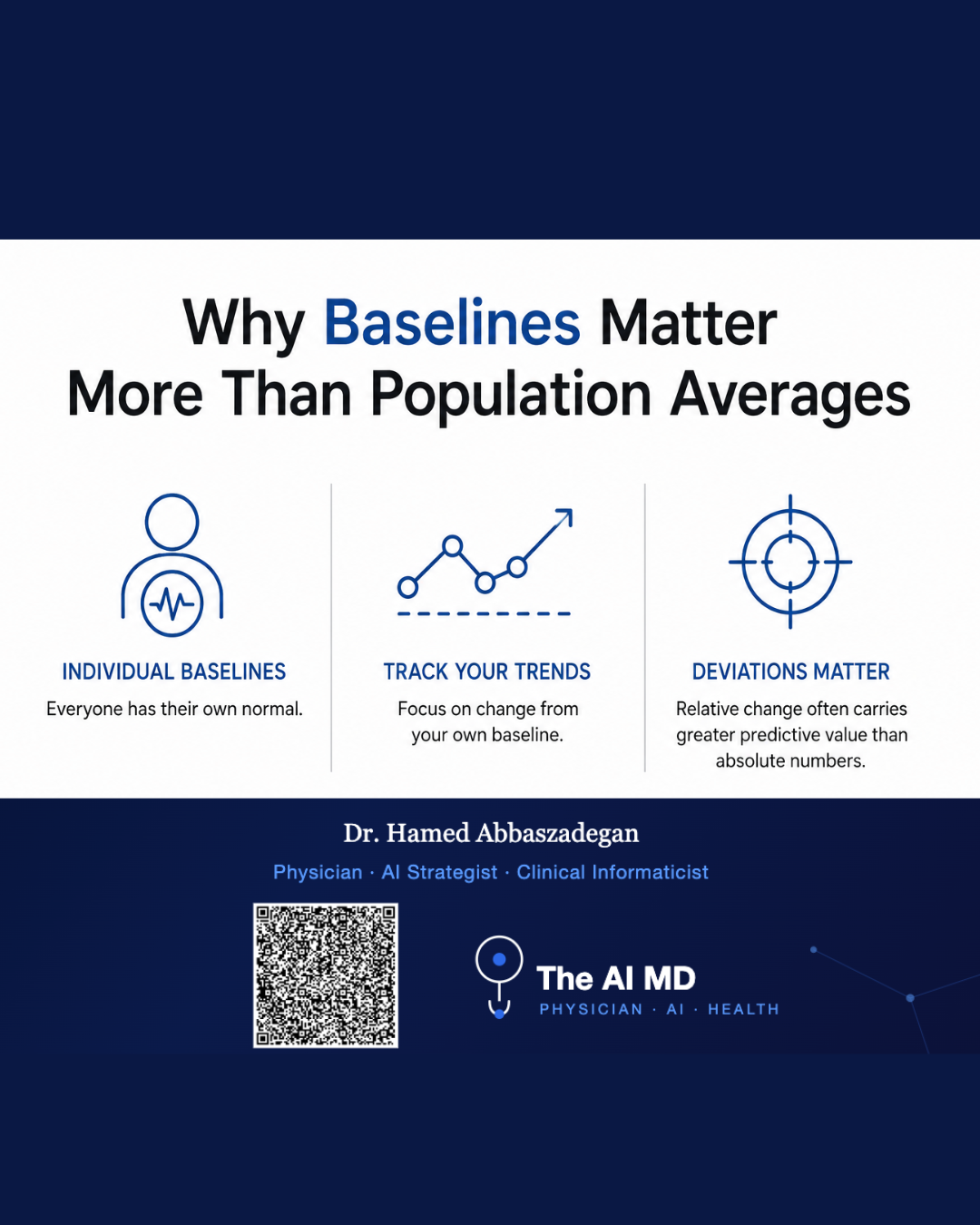
Most wearable users can't answer basic questions about their own metrics. Does better sleep follow exercise? What heart rate pattern predicts energy crashes? When does stress accumulate into metabolic dysfunction?
The gap between data collection and actionable understanding defines the current problem. People track everything and optimize nothing.
Even straightforward analysis requires complex steps. Checking data availability. Selecting appropriate metrics. Summarizing patterns across timeframes. Contextualizing findings within individual health profiles. Integrating population norms for comparison.
These steps demand robust numerical analysis combined with interpretive understanding of health. Current systems lack this capability.
The willingness-action gap proves the point. A 2022 study found 78.4% of users open to sharing wearable data with healthcare providers, yet only 26.5% actually do so. The 52-point gap reveals structural barriers preventing personal health data from reaching clinical workflows.
Healthcare providers cite concerns around data quality, validity, and the additional workload from reviewing patient-generated data outside clinical visits. Integration into electronic health records remains extremely limited. Decision support capabilities stay basic.
The infrastructure wasn't built for this. Health IT systems originated for billing and coding purposes. They don't facilitate coordination of care. They can't communicate with each other effectively. When patient-generated data enters clinical records, it gets buried with poor visibility and interpretability.
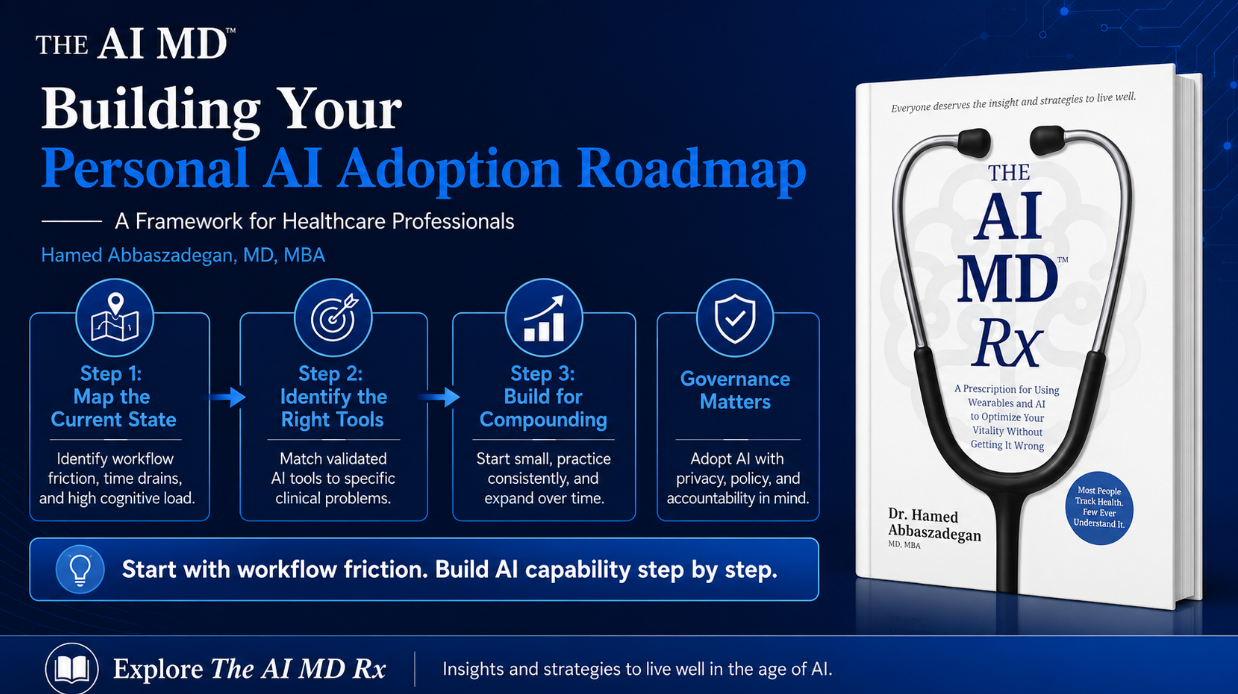
Individual agency requires new competencies.
Understanding what photoplasmography measures. Recognizing how circadian rhythm patterns affect metabolic markers. Interpreting heart rate variability trends in context of stress, sleep, and activity. Distinguishing signal from noise in continuous biometric streams.
This knowledge doesn't come naturally. Medical training takes years. Wearable users need compressed, accessible education that translates clinical concepts into practical application.
The AI MD Academy addresses this gap by providing depth of education individuals need to understand their wearables without medical backgrounds. The approach recognizes that data literacy determines whether personal health optimization succeeds or fails.
Digital health literacy disparities create unequal access. Users with more digital literacy and socioeconomic resources gain disproportionate advantages. Higher odds of using wearables associate with female gender and incomes above $75,000. Usage and data sharing decline significantly with age.
The democratization promise of wearable technology fails without addressing these literacy barriers. Technology alone doesn't transfer agency. Education does.
AI enables a fundamental reorientation from reactive treatment to predictive prevention.
Traditional medicine waits for symptoms. Labs confirm disease after pathology develops. Treatment begins when damage already exists. This model optimizes for intervention after problems manifest.
Biosimulation reverses the sequence. It models upstream biological pathways. Predicts molecular trajectories before clinical outcomes appear. Identifies intervention points years before diagnosis.
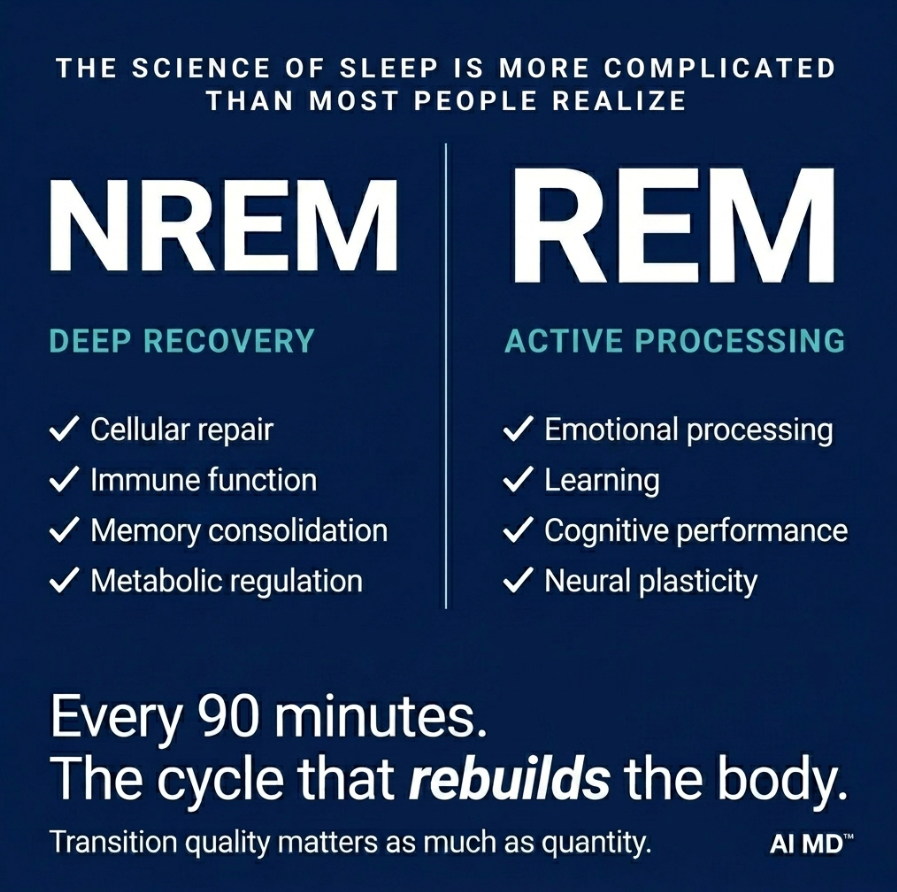
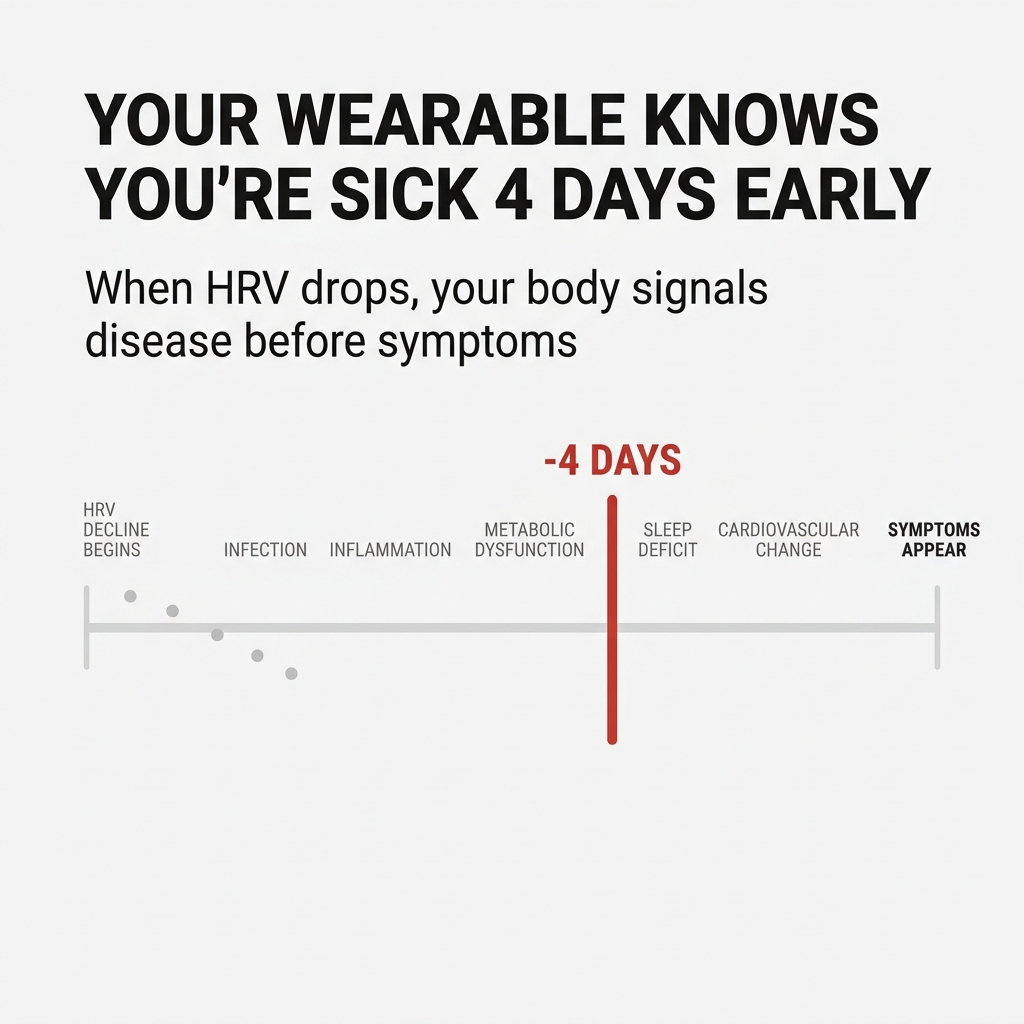
Insulin resistance leads to liver fat accumulation. Circadian misalignment triggers metabolic dysregulation. Mitochondrial dysfunction accelerates biological aging. These processes unfold over months and years before traditional lab markers detect problems.
Wearable data captures early signals. Heart rate variability patterns reveal autonomic nervous system stress. Sleep architecture shows circadian rhythm disruption. Activity trends indicate energy metabolism shifts.
AI interprets these signals in context. It simulates how current patterns project into future health states. It forecasts disease trajectories and designs interventions before pathology forms.
The shift from reactive to preventive care requires this predictive architecture. Success gets measured not by procedures performed but by diseases prevented.
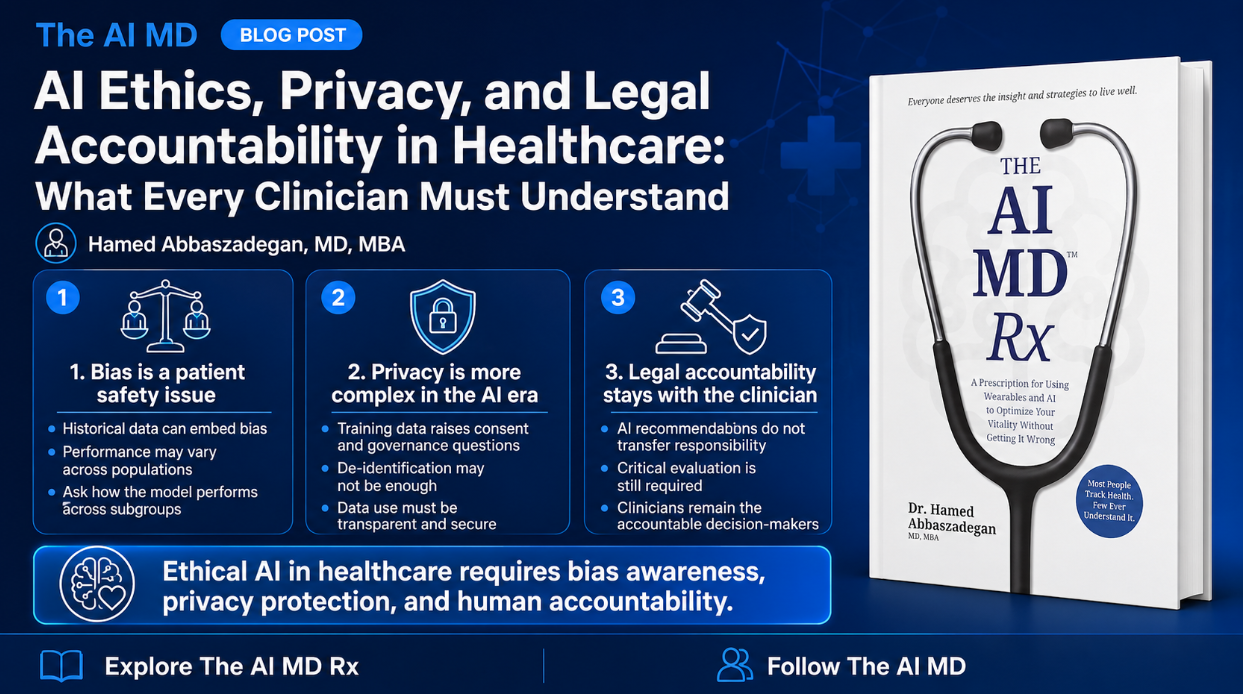
Commercial wearable devices don't fall under FDA oversight. Data not paired with doctor-patient relationships don't fall under HIPAA privacy protection. Most health metrics exist without regulation, open to sale to data brokers.
Multiple state laws now classify wearable-derived metrics like heart rate, skin temperature, and sleep as sensitive personal information. The same device used in healthcare settings may be subject to HIPAA while the identical consumer device falls under different state laws.
This convergence of federal and state regulations creates complex compliance challenges. The governance gap leaves individuals exposed.
Healthcare Standards Institute develops AI governance standards for healthcare operations. The work recognizes that speed without safety isn't progress. Standards enable scale. Governance isn't constraint—it's foundation for sustainable innovation.
The framework must address data ownership, consent models, algorithmic transparency, and bias monitoring. It needs to balance collective health benefits against individual privacy rights. Regulatory structures lag behind technological capabilities, creating uncertainty that slows beneficial innovations.
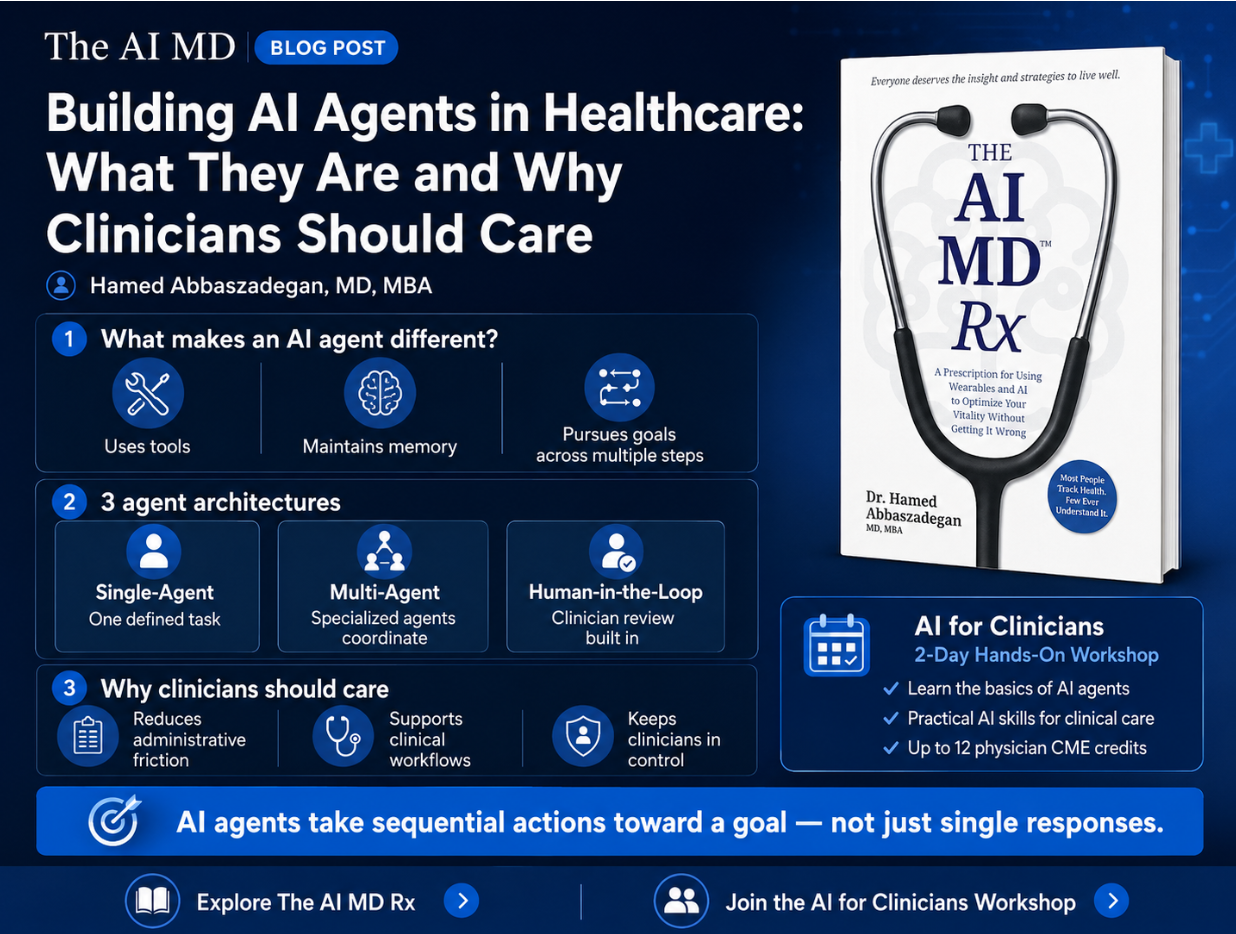
Effective implementation positions technology as collaborative tool, not autonomous decision-maker.
The human-AI partnership preserves physician judgment as final authority while providing AI-generated insights, risk scores, and evidence synthesis. Medicine involves ethical considerations, patient preferences, and contextual factors that purely algorithmic approaches can't fully capture.
Patients arrive with interpreted wearable data. Doctors review AI-generated health projections. Together they design interventions based on predicted trajectories rather than current symptoms.
This model requires training both sides. Individuals need education to interpret their data meaningfully. Clinicians need frameworks to integrate patient-generated insights into clinical decision-making.
The AI MD Academy provides videos for clinicians to learn alongside patient education. The approach recognizes that successful transition demands collaborative understanding between patients and their doctors.
Healthcare providers express concerns about data quality and validity. These concerns root in mistrust of technology and patients' ability to use tools correctly. Varying levels of digital health literacy among healthcare professionals themselves negatively impact how they interact with patient-generated data.
The partnership model addresses these concerns through structured education, standardized data formats, and clear protocols for integrating wearable insights into clinical workflows.
Current healthcare economics optimize for treatment volume. Hospitals get paid for procedures. Pharmaceutical companies profit from medications. Insurance models reimburse interventions after illness develops.
Preventive medicine disrupts these incentives. Success means fewer hospitalizations. Less medication. Reduced specialist visits. The economic model must shift from reactive treatment to proactive prevention.
AI-driven efficiency threatens jobs in medical coding, transcription, and routine diagnostics while creating demand for data scientists, AI specialists, and technology integration managers. Healthcare organizations face substantial capital requirements for AI infrastructure, advantaging large systems over small practices.
The transition period creates uncertainty for all stakeholders. New legal frameworks must address liability when AI systems contribute to medical decisions. Is the physician liable for trusting the algorithm? The hospital for implementing the system? The software developer for the underlying code?
These unresolved questions create risk aversion that prevents beneficial AI adoption. The economic realignment requires new payment models, liability frameworks, and incentive structures aligned with prevention outcomes rather than treatment volume.
AI medical technologies developed in wealthy nations may not transfer effectively to resource-limited settings with different disease profiles, infrastructure constraints, and cultural contexts.
However, AI also offers leapfrogging opportunities. Developing nations could skip traditional healthcare infrastructure investments and deploy mobile-first, AI-enabled systems.
The technology's global impact depends on intentional efforts to ensure equitable access and context-appropriate design. AI systems trained on historically biased data perpetuate existing healthcare disparities. If training datasets underrepresent certain demographic groups, resulting algorithms perform poorly for those populations.
This technical limitation has profound social justice implications. AI could either reduce health inequities by extending care to underserved populations or amplify them by embedding historical prejudices into automated systems.
Addressing this requires intentional dataset curation and continuous bias monitoring. The democratization of medical expertise through AI-powered diagnostic tools enables healthcare providers with less specialized training to deliver sophisticated care. A general practitioner equipped with AI dermatology screening can detect skin cancers with dermatologist-level accuracy.
This capability addresses the global shortage of specialists and reduces healthcare disparities between wealthy urban centers and resource-limited regions. The implication extends beyond efficiency—it fundamentally redistributes medical knowledge, challenging traditional hierarchies within healthcare systems.
People already interact with their health data differently. They want their doctors to guide them through wearable insights. The shift isn't theoretical—it's happening now.
Three years ahead, successful personal health optimization looks like this: People spot check their data. They monitor trends. They make lasting impacts to their health based on predicted trajectories rather than current symptoms.
The infrastructure to support this transition requires data literacy education, governance frameworks, clinical integration protocols, and economic realignment. None of these pieces exist at scale yet.
Building them determines whether AI medicine's revolution empowers individuals or reinforces institutional control. The technology enables the shift. The implementation choices decide who benefits.
The real revolution happens when someone understands their morning heart rate variability reading well enough to adjust their day before metabolic dysfunction accumulates. That moment relocates medical agency from the institution to the individual.
Everything else is infrastructure to make that moment possible.


%20(1880%20x%20940%20px)%20(3%20x%204%20in)%20(1).png)




.png)


Stay Connected
If you’d like these insights delivered straight to your inbox, you can sign up below. You’ll receive evidence-based perspectives on AI in healthcare, practical implementation guidance, and updates on speaking engagements and media appearances.